
TL;DR:
- Hematocrit levels reflect the proportion of red blood cells in blood, influenced by hormone replacement therapy, with testosterone raising it and estrogen lowering it. Monitoring these levels is crucial to prevent cardiovascular risks like clotting and stroke, especially in older individuals or those with underlying health conditions. Managing elevated hematocrit involves hydration, dose adjustments, formulation changes, or therapeutic phlebotomy, emphasizing personalized care based on individual risk factors.
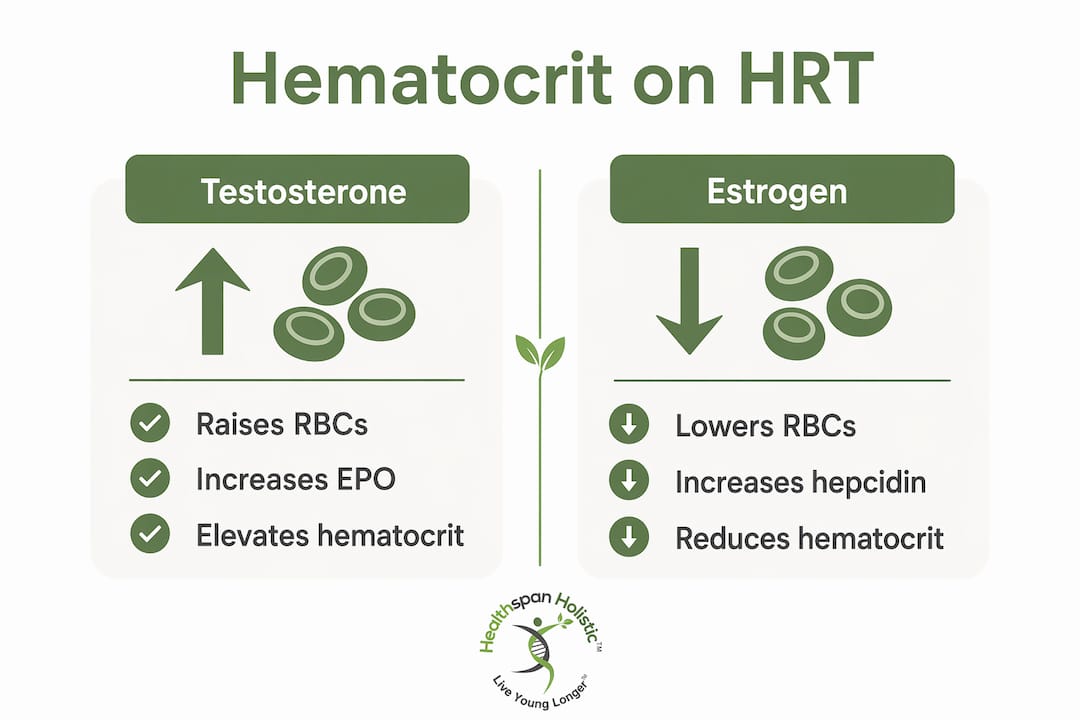
Hematocrit is defined as the percentage of your total blood volume made up of red blood cells, and it is directly altered by hormone replacement therapy. For anyone between 45 and 75 on HRT, tracking this single number can mean the difference between thriving on therapy and quietly accumulating cardiovascular risk. Testosterone raises hematocrit by stimulating red blood cell production. Estrogen does the opposite, gently suppressing it. Understanding where your levels sit, why they shift, and what to do about it gives you real control over your health while on HRT. Most providers check a complete blood count (CBC) at baseline and periodically after that. If yours does not, ask.
How does hematocrit on HRT change with testosterone vs. estrogen?
Testosterone drives hematocrit up by stimulating erythropoiesis, the process your body uses to produce red blood cells. It does this primarily by increasing erythropoietin (EPO), a hormone made in the kidneys that signals bone marrow to produce more red blood cells. The result is a measurable rise in hematocrit, often within the first 3 to 6 months of starting testosterone replacement therapy (TRT).
Estrogen works in the opposite direction. Estrogen suppresses erythropoiesis by increasing hepcidin, a protein that reduces iron availability for red blood cell production. This means people on estrogen therapy typically see stable or slightly lower hematocrit over time. The change is gradual, unfolding over weeks to months, and significant anemia is rare but worth monitoring.
The route and dose of your hormone therapy matter considerably. Intramuscular testosterone injections create higher peak blood levels than transdermal gels or intranasal formulations, and those peaks drive greater hematocrit elevation. Oral estrogen differs metabolically from transdermal estrogen, producing different effects on hematocrit outcomes as well.
Here is a quick summary of how each hormone type typically affects your blood:
-
Testosterone (TRT): Raises hematocrit through EPO stimulation; effect is dose and route dependent
-
Estrogen therapy: Lowers or stabilizes hematocrit through hepcidin increase and reduced iron availability
-
Gender-affirming hormone therapy: Demonstrates both effects clearly, with trans women on estrogen seeing hematocrit drop toward female reference ranges over months
-
Progesterone: Has minimal direct effect on hematocrit but may modulate estrogen’s impact
Pro Tip: If you are on testosterone therapy and your hematocrit is creeping up, ask your provider whether switching from weekly intramuscular injections to more frequent smaller doses or a transdermal application could reduce those peaks without sacrificing your therapy benefits.
What are the health risks of abnormal hematocrit levels on HRT?
Elevated hematocrit thickens your blood, and thicker blood moves more slowly through your vessels. That slowdown raises the risk of clots, stroke, and cardiovascular complications. The American Urological Association and the Endocrine Society use clear thresholds to guide clinical decisions. Hematocrit below 50% is generally considered safe on TRT. Levels between 50% and 54% require closer monitoring. Above 54%, clinical intervention is warranted. For patients with existing cardiovascular risk factors, some clinicians act at 52%.
Symptoms of elevated hematocrit are easy to dismiss as general aging or stress. Watch for:
-
Persistent headaches, especially in the morning
-
Dizziness or lightheadedness when standing
-
Brain fog and difficulty concentrating
-
Facial flushing or a reddish complexion
-
Fatigue that does not improve with rest
“Individual cardiovascular risk, including age, history of clots, and hypertension, guides hematocrit management decisions beyond fixed thresholds. Clinicians tailor intervention based on comprehensive risk profiles rather than strict hematocrit cutoffs.” — HRT After 55
This matters especially if you are over 60. At that age, the cardiovascular system is less forgiving of elevated blood viscosity, and the margin between therapeutic benefit and risk narrows. A 65-year-old with a history of hypertension and a hematocrit of 53% needs a different conversation with their provider than a healthy 48-year-old at the same level.
One frequently overlooked contributor is sleep apnea. Untreated sleep apnea causes chronic low-grade oxygen deprivation, which triggers the same EPO response as testosterone, pushing hematocrit higher. Dehydration is another hidden culprit. If your blood volume drops due to poor fluid intake, your hematocrit reading rises without any real increase in red blood cells. Always consider these factors before attributing a high reading entirely to your hormone therapy.
How can you manage elevated hematocrit during hormone replacement therapy?
Managing hematocrit on HRT starts with identifying the cause before reaching for a medical intervention. A stepwise approach protects you from unnecessary procedures while addressing the real driver.
| Management strategy | When to use it | Expected outcome |
|---|---|---|
| Improve hydration | First step when hematocrit is mildly elevated | Can normalize falsely high readings within days |
| Treat sleep apnea | When OSA is suspected or confirmed | Reduces EPO-driven erythrocytosis over weeks |
| Reduce testosterone dose | Hematocrit 50-54% on TRT | Gradual reduction over 4-8 weeks |
| Switch to transdermal or more frequent dosing | Persistent elevation despite dose reduction | Reduces peak levels and hematocrit spikes |
| Therapeutic phlebotomy | Hematocrit above 54% or symptomatic | Removes 500 mL blood, reducing hematocrit by ~3 points |
| Temporary treatment hold | Critical elevation with symptoms | Allows rapid normalization before resuming |
Therapeutic phlebotomy removes approximately 500 mL of blood per session and typically reduces hematocrit by about 3 percentage points. A person at 57% can expect to come down to around 53% to 54% after one session. Sessions are often repeated every 3 to 6 months depending on how quickly levels rebound.
Regular blood donation serves a similar purpose and carries the added benefit of reducing cardiovascular risk. Blood donations reduce heart attack risk by up to 88% in non-smokers, though eligibility varies and medical oversight is recommended for anyone with complex health histories. Your provider can help determine whether donation is appropriate for you.
Pro Tip: Before your next blood test, drink at least 16 oz of water in the two hours prior. Dehydration can falsely raise your hematocrit reading and lead to unnecessary interventions. Pair this with tracking your BUN/creatinine ratio on your lab results as a quick hydration check.
For men on testosterone, exploring men’s hormone health resources can help you understand the full picture of managing TRT side effects, including hematocrit, as part of a broader vitality strategy.
What is the role of blood viscosity in cardiovascular health on HRT?
Blood viscosity is the measure of how thick and resistant your blood is to flow. Think of it as the difference between water and honey moving through a tube. High viscosity means your heart works harder to push blood through your vessels, and that sustained effort increases cardiovascular strain over time.
Hematocrit is the single largest contributor to blood viscosity, but it is not the only one. Blood viscosity is influenced by hydration status, plasma proteins, white blood cells, and fatty acids in the bloodstream. This means a person with normal hematocrit can still have dangerously high blood viscosity if other factors are out of range. Focusing solely on hematocrit misses the full picture.
Key contributors to blood viscosity beyond red blood cells:
-
Hydration status: Dehydration concentrates all blood components, raising viscosity rapidly
-
Fibrinogen and plasma proteins: Elevated levels increase clotting tendency and viscosity
-
White blood cells: Elevated counts, as seen in chronic inflammation, add to resistance
-
Triglycerides and fatty acids: High levels thicken plasma and slow circulation
-
Hematocrit itself: Still the dominant factor, especially when above 50%
Lifestyle choices directly affect these contributors. Regular aerobic exercise improves red blood cell flexibility, making them better at squeezing through small vessels. A diet low in processed fats reduces triglyceride load. Staying well hydrated keeps plasma volume up and viscosity down. These are not minor tweaks. They are the foundation that makes your HRT safer and more effective.
A comprehensive blood panel that includes hematocrit, CBC, lipid panel, and inflammatory markers gives you and your provider the full picture of what your blood is doing, not just one slice of it.
How to monitor and maintain healthy hematocrit levels during HRT
Monitoring hematocrit levels during HRT follows a clear schedule that most people can track alongside their regular appointments.
-
Baseline test before starting HRT to establish your personal reference point
-
3 to 6 weeks after starting or after any dose change, to catch early shifts
-
Every 3 to 6 months during the first year of therapy
-
Annually once levels are stable and within a safe range
Interpreting your CBC results means looking at hematocrit alongside hemoglobin and red blood cell count. A rising hematocrit paired with rising hemoglobin confirms true erythrocytosis. A rising hematocrit with stable hemoglobin and a high BUN/creatinine ratio points more strongly toward dehydration as the cause.
Recognizing when to call your provider matters as much as the monitoring itself. Contact your care team if your hematocrit exceeds 52%, if you develop new headaches, vision changes, or shortness of breath, or if your symptoms change significantly after a dose adjustment.
Pro Tip: Keep a simple health log noting your hematocrit result, your hydration habits that week, and any symptoms. Over time, this gives you and your provider a pattern to work with rather than isolated data points.
Lifestyle habits that support healthy hematocrit include drinking at least 8 cups of water daily, prioritizing 7 to 9 hours of sleep, getting screened for sleep apnea if you snore or wake unrefreshed, and eating iron-rich foods in moderation rather than supplementing iron aggressively without testing. Women on testosterone therapy should be aware that even low-dose testosterone can raise hematocrit, making monitoring just as relevant for them as for men on TRT.
Key takeaways
Managing hematocrit on HRT requires regular monitoring, individualized risk assessment, and a willingness to adjust therapy before problems escalate.
| Point | Details |
|---|---|
| Testosterone raises hematocrit | TRT stimulates EPO and red blood cell production; monitor CBC within 3-6 weeks of any dose change. |
| Estrogen lowers hematocrit | Estrogen increases hepcidin and suppresses erythropoiesis gradually over weeks to months. |
| Risk thresholds guide action | Below 50% is safe; 50-54% requires monitoring; above 54% requires clinical intervention per AUA and Endocrine Society guidelines. |
| Dehydration distorts results | Always hydrate well before testing and check BUN/creatinine ratio to rule out false elevation. |
| Management is stepwise | Start with hydration and lifestyle, then adjust dose or formulation, then consider phlebotomy if needed. |
Chris’s take on hematocrit and HRT after 50
Here is something I see consistently: people over 55 on hormone therapy who feel great but have never had their hematocrit checked beyond the initial baseline. Their providers are focused on symptom relief, and the blood work quietly slides. That is a gap worth closing.
What I have come to believe is that hematocrit is not just a safety checkbox. It is a window into how your body is responding to therapy at a cellular level. When it climbs, it is telling you something, whether that is that your dose is too high, your hydration is poor, your sleep apnea is untreated, or your cardiovascular system needs more support.
The older you are, the more that signal matters. A 68-year-old with a hematocrit of 53% and a history of high blood pressure is in a different category than a 50-year-old with the same number and no risk factors. Individualized management is not a luxury. It is the standard of care.
What I encourage everyone reading this to do is bring your last CBC to your next appointment and ask specifically about your hematocrit trend, not just the single number. Trends tell the real story. And if your provider is not tracking it routinely, you now have the knowledge to ask for it. That conversation could protect your heart and brain for decades to come.
— Chris
Support your blood health with Healthspan Holistic
If you are on HRT and want to stay ahead of hematocrit and cardiovascular risk, targeted lab testing is the smartest first step. Healthspan Holistic offers the Magnesium RBC Test to detect deficiencies that affect red blood cell health, the Cellular Micronutrient Test to assess the nutrients driving red blood cell production, and the Basic Heart Health Test for cardiovascular risk screening that pairs directly with hematocrit monitoring.

Our professional-grade supplements support hormone balance, antioxidant protection, and cardiovascular wellness. 1st Time Customers can take advantage of our BUY 1 GET 1 50% OFF special offer on all supplements. Pair your testing with personalized coaching to build a blood health plan that works alongside your HRT, not against it.
FAQ
What is a normal hematocrit level on HRT?
Normal hematocrit on HRT depends on your hormone type and sex. For men on testosterone, levels below 50% are generally considered safe, with clinical intervention recommended above 54% per American Urological Association guidelines.
Is hematocrit affected by estrogen therapy?
Yes. Estrogen typically lowers or stabilizes hematocrit by increasing hepcidin and suppressing red blood cell production. The effect is gradual, taking weeks to months, and varies with dose and whether estrogen is taken orally or transdermally.
Can dehydration cause a false high hematocrit reading?
Dehydration concentrates your blood, raising hematocrit without any true increase in red blood cells. Drinking water before your blood draw and checking your BUN/creatinine ratio helps distinguish real erythrocytosis from a hydration artifact.
How often should hematocrit be checked on HRT?
Check hematocrit at baseline, 3 to 6 weeks after starting or changing your dose, every 3 to 6 months in the first year, and annually once stable. More frequent checks are warranted if levels are trending upward or symptoms appear.
What does therapeutic phlebotomy do for high hematocrit on TRT?
Therapeutic phlebotomy removes approximately 500 mL of blood per session, reducing hematocrit by about 3 percentage points. It is typically repeated every 3 to 6 months and is recommended when hematocrit exceeds 54% or when symptoms of hyperviscosity are present.
Leave a comment: